
Women and Pain: Taking Control and Finding Relief
PAIN DEFINED
The Burden of Chronic Disease
Pain is “an unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage…Pain is always subjective…It is unquestionably a sensation in a part or parts of the body, but it is also always unpleasant and therefore also an emotional experience.”
If you have chronic pain, you’re not alone. An estimated 25.3 million adults in the United States report severe, daily pain, significantly more women than men, while 55 percent of U.S. adults report at least some pain in the past three months. 1 Chronic pain is one of the most frequent reasons for physician visits and among the most common reasons for taking medication. 2
But there’s a gender gap when it comes to pain. Women have more frequent, longer lasting, and severe pain than men. 1 3 For instance, one national survey found that while about 16 percent of white men and 8 percent of black men reported severe pain, those numbers jumped to about 22 percent for white women and 11 percent for black women, respectively. 1
Women are also more likely to develop painful diseases, such as chronic fatigue syndrome, fibromyalgia, endometriosis, interstitial cystitis, vulvodynia, and temporomandibular disorders (TMJ) than men. They also report greater pain severity than men from certain conditions, such as cancer. 2 And women simply pay attention to pain from physical conditions more than men. They recognize when something is wrong. Men, on the other hand, have a tendency to ignore pain when they should pay attention to it.
Women also differ in their response to pain medications. They tend to need higher amounts of pain medications immediately after surgery, while men tend to use more pain relievers later in the recovery period. 4 Conversely, some medications (the partial kappa-opioid agonists, such as nalbuphine [Nubain] and pentazocine [Talwin]), can provide greater pain relief in women than men, although opioids such as morphine and codeine can lead to more nausea and vomiting in women than men. 5-7
The question that has plagued researchers for decades is: “Why?”
Part of it could be anatomy. Women have more nerve receptors than men, so they may be hard-wired to feel more pain. 8 Even something as seemingly minor as the thickness of your skin or the size of your body can affect pain perception. 9 Another reason may be that women are more likely to see a doctor than men, so maybe they’re just getting diagnosed more often.
Genetics also plays a role, affecting how long neurons that transmit pain signals to the brain survive and the strength of pain response, as well as pain tolerance, perception, and response to pain relievers. 2 But we also know that reproductive hormones—estrogen and progesterone in women, testosterone in men—play a role in these pain-related gender differences.
In women, the continual variation of hormonal levels through puberty, menstruation, pregnancy, and pre- and post-menopause contribute to these sex differences. For instance, prior to puberty, there are no significant differences in the development of painful conditions between boys and girls. 10 Afterward, the differences are dramatic, with women two- to six-times more likely to develop chronic pain conditions, such as headaches, irritable bowel syndrome, and fibromyalgia.11 There are also differences in pain levels and frequency after menopause.
Pain intensity tends to increase when estrogen levels are low and progesterone levels are high, as they are during the second half of the menstrual cycle, possibly because there are more naturally occurring “feel good” chemicals in the brain when estrogen levels are high. 5 12 You can imagine the evolutionary benefit to this: estrogen levels are highest during pregnancy and childbirth, thus providing some natural pain relief. Indeed, during pregnancy, when levels remain high and steady, studies indicate many pain conditions improve and pain sensitivity is lower. 10 11
Meanwhile, one interesting study found that women with TMJ reported less pain as pregnancy progressed (and estrogen levels rose) and more pain after surgical menopause (when estrogen levels plummet). 13 There’s even a name for it: pregnancy-induced analgesia. 10
In addition, reproductive hormones can also influence how well opioids and other pain relievers work. 14
But What About Men?
Although this resource speaks to specific issues facing women living with pain, A Guide to Optimizing Treatment through Integrative Health for People Living with Pain, is available at drwaynejonas.com/painguide and addresses whole-person pain care in both women and men.
The Menopausal Transition and Pain
Surprisingly, there is little research on the effects of the pre-menopause transition, called perimenopause, and menopause on pain severity and frequency.47 But we are beginning to learn.
One study of 101 women seen in a menopause clinic in Italy, all of whom had some form of chronic pain (headaches, fibromyalgia, arthritis, back, or abdominal pain), found that about 18 percent said their pain started after menopause; about 17 percent said it stopped after menopause; and the rest said their pain that had begun prior to menopause continued after the transition. As might be expected with age, arthritic pain started or got worse after menopause in half the women. 47
Indeed, musculoskeletal pain, such as arthritis and back pain, have some connection to hormonal levels, with evidence that estrogen can affect the cartilage and fluid around the joints. This could explain why women tend to have more severe knee arthritis after menopause than men of a similar age. 48 An analysis of seven studies also found a much greater prevalence of back pain during the perimenopausal period than either before or after menopause. 49
Another interesting finding is that women with high-intensity, high-frequency pain reported that their pain improved or remained stable after menopause, while those with low-intensity and less extended pain said it got worse. The authors of this study concluded that “menopause can act as a determinant in the evolution of painful conditions.” Translation: your pain may get better or worse after menopause, depending on its cause and severity. 47
One area where it might get worse is migraines. A recent study found that women were 60 percent more likely to experience 10 or more migraines a month during the perimenopausal period than before. It didn’t get any better after menopause; women reported their headaches’ frequency increased 76 percent. 50
Finally, a study presented at the 2017 North American Menopause Society annual meeting found that female veterans in the perimenopause phase were 85 percent more likely to be diagnosed with chronic pain than younger women. They were also more likely to be taking opioids. As the author concluded: “[These findings] support the idea that menopause transition may be an under recognized period of risk for chronic pain, as well as for high-risk opioid use. We may be able to think of menopause as kind of a sentinel event in some way for more difficulty with experiencing these symptoms, or for management of these symptoms, or kind of just additional needs.” And those considerations, she said, should impact how clinicians deliver care to these women, “thinking about what it is that we’re really treating and how these treatment decisions affect health in the menopause transition and as women are aging.” 50
LIFE EXPERIENCES AND EMOTIONAL STATUS
A woman’s past experiences, particularly those involving trauma and abuse, as well as her current emotional state and life stresses, have an enormous impact on her level of pain and even the development of painful conditions. Indeed, I often think of chronic pain as a sign that these experiences are embedded in your body, and pain is the means by which your body responds to those traumas, even if they happened a long time in the past.
Before I say anything else on this, however, let me also say that no matter your past history, your pain is real. It’s just that your past history may increase your body’s response to pain and make you more susceptible.
One study of 380 women found that those who reported they had been victims of bullying or abuse were more likely to experience painful genital/urinary conditions. 15 What happens is that their body remains on high alert. In most people, the normal response to pain is that the body adjusts and the pain diminishes. But in people with a history of trauma, the body exists in constant “alert” mode, leading to a hyperawareness of external and internal stressors.
Even socioeconomic status and work environment can impact the perception of pain. 16
This is why it is so important that you work with your health care team to identify issues beyond the physical—including the emotional, social, mental, and spiritual—to help you.
Women and Opioids
The opioid epidemic in this country has been termed a public health crisis. More than 250 million prescriptions are written for opioids each year. And while the amount of prescription opioids sold nearly quadrupled from 1999 to 2010, the amount of pain Americans reported remained unchanged. Since 1999, the number of overdose deaths involving opioids (including prescription opioids and heroin) quadrupled. Today, 91 Americans die every day from an opioid overdose, many from prescription opioids. 17
Many of those dying are women (Figure 1). Indeed, about 18 women die every day from a prescription painkiller overdose. Between 1997 and 2015, the rate of deaths from prescription opioid overdoses increased 471 percent among women, compared to 218 percent among men. 18 19
A recent study found that women ages 40 to 59 are prescribed more opioids than any other age group and receive twice as many opioid prescriptions as men. About 13 percent of middle-aged women prescribed opioids after surgery will still be using them three to six months after surgery, putting them at high risk for addiction. This age group also has the highest death rates from opioids. 2
Figure 1. Drug Overdose Deaths Among Women
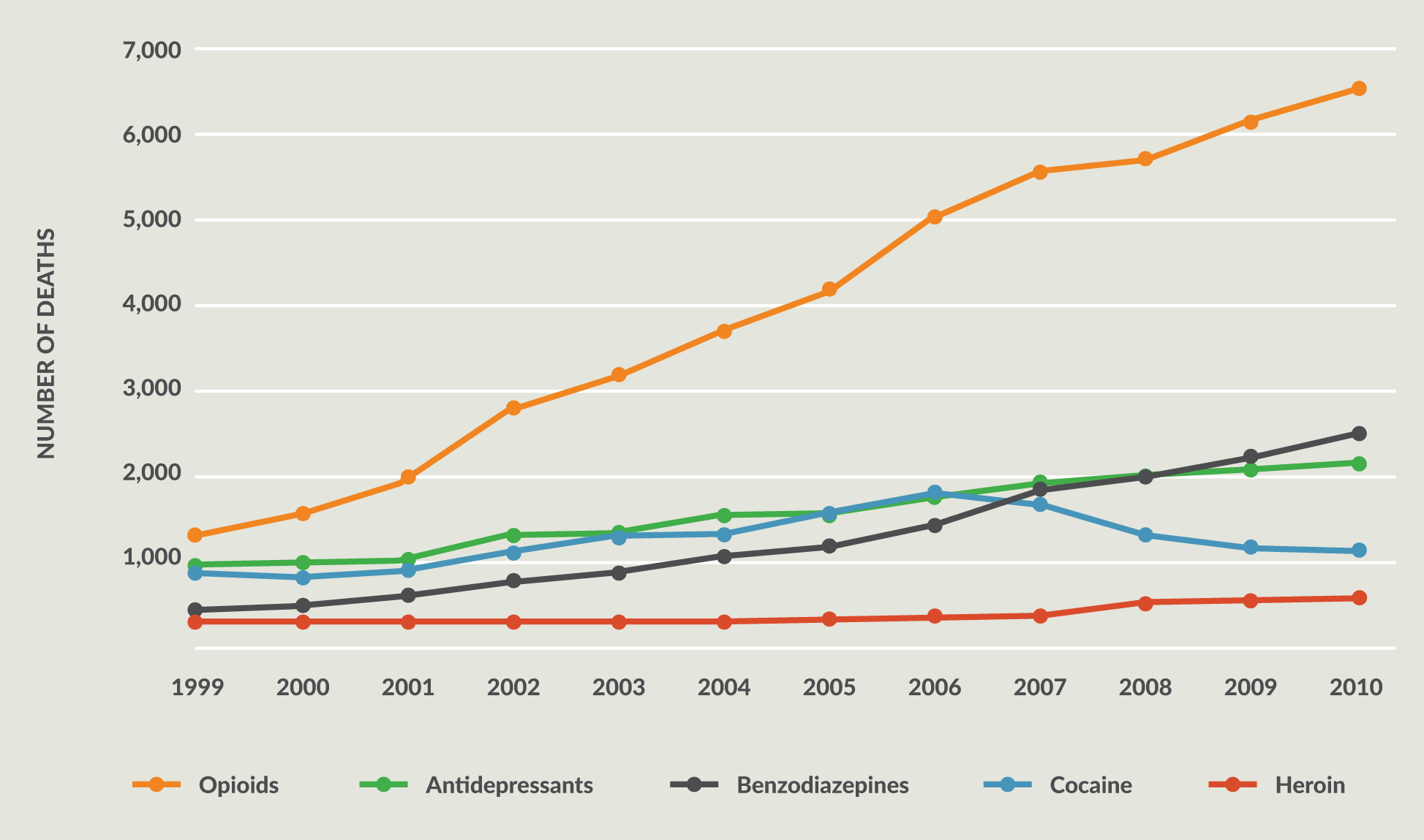
Quintiles IMS. An Analysis of the Impact of Opioid Overprescribing in America: Pacira Pharmaceuticals; September 2017.
Women are also using more opioids during pregnancy, putting their infants at risk of dependence and post-partum withdrawal. This, in turn, has led to what experts call an epidemic of infants born already dependent on opioids, who then have to go through a painful withdrawal process. 21 22
While opioids definitely have a place in the treatment of acute pain (such as after surgery or accidents) and in palliative care (such as during a sickle cell crisis or near the end of life), the Centers for Disease Control and Prevention and other medical organizations recommend starting with non-opioid alternatives as a first-line treatment for chronic pain, including acetaminophen (Tylenol), nonsteroidal anti-inflammatories (i.e., Motrin, Aleve), antidepressants, and anticonvulsants, and non-drug approaches such as yoga, manipulation, acupuncture, massage, and mind-body methods. 2
FACING DISCRIMINATION
Numerous studies dating back decades attest to the fact that the medical system does not take women’s pain seriously, whether chronic or acute. 24 For instance, a 2011 report from the National Institutes of Health found that medical professionals were more likely to dismiss women’s reports of pain. 2
An oft-quoted study of 981 men and women seen in the emergency room found that women were 13 to 25 percent less likely to receive strong pain medication, despite the fact that they had the same pain scores as men and waited about 16 minutes longer to get medication. 25 Women with endometriosis, an extremely painful reproductive condition, often go years before getting a diagnosis. They are told their excruciating pain is a normal part of menstruation, or even that it is all in their heads—and are prescribed antidepressants. 26
Meanwhile, a 2015 survey of more than 2,400 women with chronic pain, most with fibromyalgia and/or back pain, conducted by National Pain Report and For Grace, a non-profit organization, found that more than 90 percent of those with chronic pain thought the system discriminates against women with pain, with 65 percent saying they thought doctors took their pain less seriously. The survey also found that women believe there is a gender bias in how doctors treat their pain (Figures 2 and 3). Interestingly, it didn’t seem to matter if the doctor was male or female. 27
Figure 2.
Do you feel you are treated differently by doctors because you are a woman?
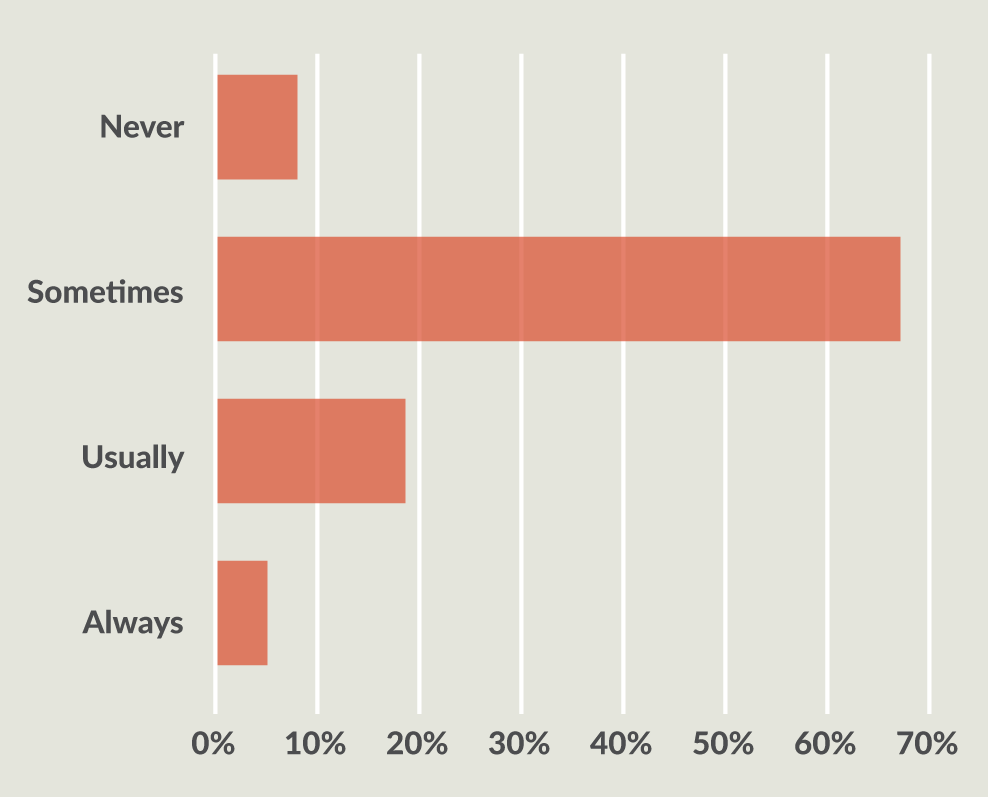
Figure 3.
Do you think the health care system discriminates against female patients?
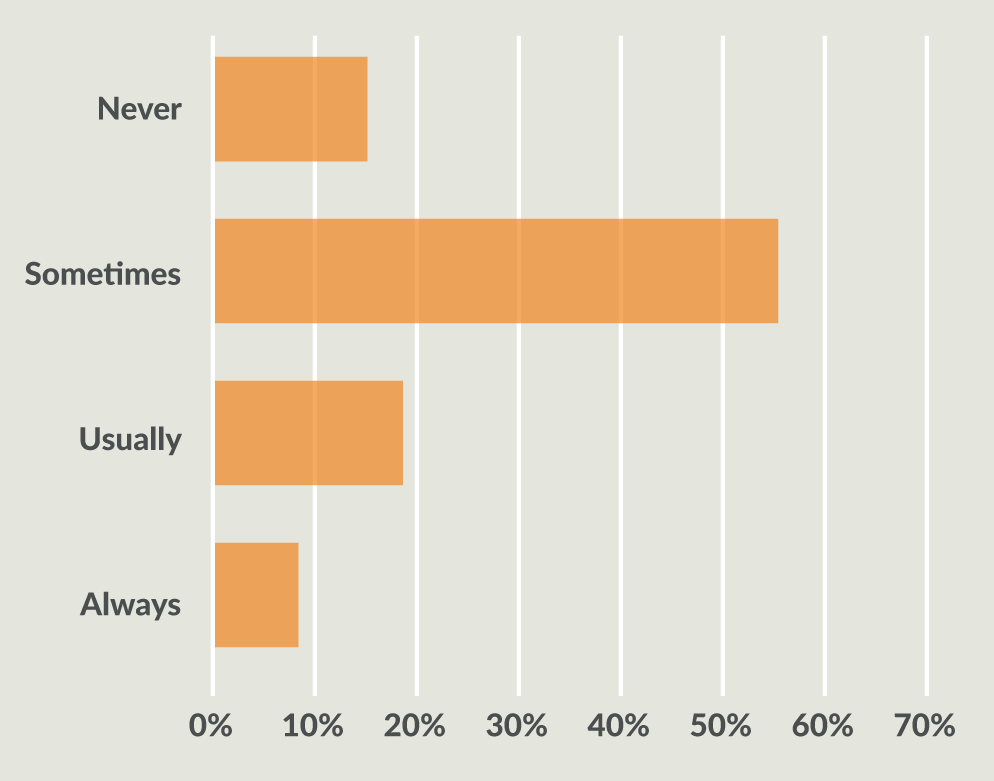
Source: Women in Pain Survey. 2015. https://www.surveymonkey.com/results/SM-P5J5P29L/.
In addition, 75 percent of the survey respondents said their doctors told them they had to learn to live with the pain. More than half said their doctors didn’t know what was wrong with them, while 52 percent said they were told that since they “looked good,” they must be feeling better. Forty-five percent were told that the pain was all in their head. 27
This is why it’s so important that you take a proactive role in finding the right doctors and other health care practitioners to work with. You have to advocate for yourself at a time when your energy and drive may be sapped by the pain. If you can’t do this on your own, bring someone with you to appointments and have them help you research providers to find those who will listen to you and provide the evidence-based care you deserve. Ideally, that will be an integrative medicine physician, where I think you’ll find your best chance of being listened to, believed, and treated with respect.
Keep in mind, though, that communication goes both ways. While you should expect your doctor to communicate openly with you, respect your goals and decisions, and take your pain seriously, you also have a role. You must engage in your own self-care for health.
My advice is to keep a pain diary for at least a week before your visit in which you rate your pain every couple of hours on a scale of 1 to 10, noting what you were doing or thinking when it occurred. When talking with your doctor, focus on the impact the pain has on your life (i.e., it prevents you from exercising or going to work), not just the pain itself. And be specific when defining the pain in terms of the location, intensity, and when it is worst. Also list the non-drug behaviors that help relieve the pain and improve function, including sleep, movement, diet, and stress management. Then bring that list with you when you see your health professional. It will make the visit more productive and help you both better understand your pain and how it impacts your life.
Getting it Down in One Place
Even with the advent of electronic health records, it’s still a good idea to keep track of your medical history yourself. This includes tracking emergency contact information, diagnoses, current treatments (including prescription and over-the-counter medications and supplements), and allergies. You can find a sample here.
Who is Treating Your Pain?
You may see several physicians as you search for pain relief. These include:
- Primary care physicians. Pain is one of the main reasons people see their primary care physicians. They treat all conditions and should view your condition holistically.
- Pain management specialists. These physicians often are trained in anesthesia with additional training in pain management. They include interventional anesthesiologists, who can implant pumps and other devices to help relieve your pain.
- Neurologists. These physicians focus on the central nervous system. They are most likely to treat neuropathic pain (pain related to the nerves).
- Orthopedists and sports medicine doctors. These physicians address the skeletal system, including bones, joints, and tendons.
- Rheumatologists. These physicians address the immune system. They are likely to treat people with painful autoimmune diseases such as lupus, scleroderma, and fibromyalgia.
Ideally, you will also see complementary health providers trained in pain management. These include:
- Chiropractors. Chiropractors see approximately 40 percent of chronic pain patients, with one study finding that about a third of patients with chronic back or neck pain turned to a chiropractor. 28 A survey from Consumer Reports found that 59 percent of people with chronic pain who saw a chiropractor were highly satisfied, compared to 34 percent who saw only a primary care physician. 29 30
- Acupuncturists. There is good evidence of the long-term benefits of acupuncture on chronic pain. 31 One study found that acupuncturists treat about 7 percent of chronic pain patients. 28
- Physical therapists. Physical therapists specialize in restoring function to patients with chronic pain. For instance, if you have arthritis of the knee, they work with you to strengthen the muscles that surround the knee, which can help with the pain.
- Massage therapists. About half of those who get a massage every year are doing it for some medical reason, primarily pain relief, or soreness and stiffness. One survey of more than 1,000 adults found that 89 percent believed that massage was effective in reducing pain, with 28 percent stating they used massage therapy for pain relief. 32
- Cognitive behavioral therapist (CBT). Dozens of studies attest to the benefits of this psychological approach, in which you work with a therapist to reframe how you think about and react to your pain.33
Don’t limit yourself to just one type of provider. When it comes to treating chronic conditions such as pain, an integrative approach merging the traditional and the alternative is best. One way to think of this is “transformative care.” But in addition to receiving treatment from the health care professional, this approach also requires that you participate in self-management strategies, such as mindfulness-based stress reduction techniques including meditation, massage, and yoga, as well as lifestyle management, including getting enough sleep, following a healthy diet, exercising, and engaging in healthy social activities. 34
You can learn more about integrative approaches at www.drwaynejonas.com
MANAGING PAIN
Managing chronic pain requires a holistic approach of medical and complementary therapies. A 2015 survey of 2,400 women with chronic pain found that 65 percent had tried exercise; 49 percent massage; 45 percent physical therapy; and 42 percent meditation for their pain. Many also tried yoga (27 percent), chiropractic (26 percent), acupuncture (20 percent), and medical marijuana (18 percent). 27
One area that is important and should not be neglected is how you think about your pain. One study found that women with negative thoughts about their pain—who magnify the pain in their minds—report more severe pain and are more likely to be taking prescription opioids than men with the same painful condition or women with lower levels of negative thinking. 35
This is where cognitive behavioral therapy can be particularly helpful. This form of short-term therapy teaches you to put your pain into the proper context and veer away from negative thoughts. Studies show it is quite effective at treating chronic pain and reducing catastrophizing, with or without other approaches. 36 37
Depression and Pain
If your doctor, family, or friends tell you that you seem depressed, they might be right. Pain and depression often go hand in hand, with pain both a symptom and a cause of depression. That doesn’t mean the pain you feel isn’t real or that it’s “all in your head.” In fact, headaches, body aches, and back pain are all symptoms of possible depression. So don’t let anyone minimize the pain you’re feeling. For while there’s a large emotional component to pain that the medical profession might separate out as depression or anxiety, it doesn’t matter if the pain is physical or emotional; it’s the cross link that’s real, and it leads to real impairment. In fact, true remission only occurs when you treat both the emotional and the physical symptoms of depression. 44
That’s why I consider it so important when I see a patient with pain to assess her as a whole person—not just focusing on her pain.
One aspect that often gets ignored is the social aspect of pain. When you’re in pain, you tend to withdraw from your normal activities. This means withdrawing from people—and the people you love withdrawing from you. The isolation this creates can be devastating because social support is essential to health and healing. Indeed, without a social network, stress hormones surge, triggering the release of inflammatory chemicals and activating genes that can damage the mind and body. This includes slowing the healing process and preventing restorative sleep. 38 39
Another important component is self-care. Women are famous for pouring all their energy into caring for others and very little into caring for themselves. This is what happened to Carol, a 47-year-old patient of mine. She had been doing really well with her self-care—eating right, exercising, finding time to do the things she enjoyed and saying no to those she didn’t—but then her 10-year-old son was diagnosed with a mental health condition, and her own self- care went out the window. She started gaining weight and stopped her stress management program Then she was in a car accident and hurt her neck. What should have been a short-term issue turned into a chronic pain condition.
Working together, we identified a safe, quiet place in her house where she could go to be alone and do whatever she liked. She called it “My Space.” Simply carving out that time for herself helped her see how she had lost her way, and gradually she was able to reintegrate the other lifestyle approaches she needed to return to a healthier—and pain-free—life.
Pain During Labor
There is no minimizing the magnitude of the pain of giving birth. But there are non-pharmaceutical ways to minimize the pain itself. A review of 11 randomized, controlled trials conducted with 1,374 women found that relaxation techniques and yoga could reduce the pain of labor, increase satisfaction with childbirth, and lower rates of instrument-assisted vaginal delivery. 45
Another analysis of five trials on self-hypnosis during labor found it reduced the need for pain medications—including epidurals—and left women more satisfied with their pain management compared to women who did not use hypnosis.12 There is also good evidence for the pain-relieving properties of acupuncture during delivery, with studies finding that women who use it during labor are less likely to use other types of pain relief; have less pain and fewer instrument deliveries; and are more relaxed and have a greater sense of control. Acupressure also provides pain relief. 46
TIME TO JOURNAL
Journaling is a way of going on a retreat without leaving your home. It is a way to access and acknowledge past experiences that may be causing you pain and reintegrating them into your life so they become a part of you. It helps bring order to your deepest thoughts and fears and enables you to learn from the person who knows you best: you. Plus, you can go back and read what you’ve written to see how much progress you’ve made. Bottom line: Journaling provides a safe environment that enables you to face your traumas. When that happens, remarkable healing follows. Indeed, studies find that journaling can reduce pain, improve depression, and even lower markers of inflammation. 40-43
Journaling can also provide clues as to what makes your pain worse. For instance, one of my chronic pain patients, Mary, started keeping a journal in which she wrote down observations about what made her feel well and what did not. They didn’t have to be linked to her pain. It could be anything she saw that helped her feel better about herself—helped her feel happy and well. After two months of keeping this journal, she returned with several insights.
First, her back felt worse when she did not get enough sleep. Her normal pre-bed routine was eating a bowl of ice cream while watching the news, then reading on her iPad for 20 minutes before turning out the light. We talked about the stress that watching the news could trigger and the fact that the late-night snack could make for a less restful sleep as her body digested the food. Reading her tablet, with its “blue light,” is a known sleep deterrent.
So Mary began a sleep hygiene program that involved some calming tea before bed and five minutes of sitting quietly. When she got into bed, she read a real book before turning out the light and kept her phone and other electronics out of the bedroom. The result? Her sleep improved, leading to less pain on the days she followed this routine.
She realized other things through journaling as well. When she did her stretching and physical therapy exercises she definitely felt better. But she had been doing them sporadically. After seeing the pattern, she made them a priority first thing in the morning. She also learned something else: On the anniversary of her father’s death, she felt excruciating pain. “Maybe I haven’t truly dealt with his death,” she said to me. So she started therapy to explore that issue.
My point is that the act of writing things down—with a pen and paper, not a phone or computer—can help you see the influences of your current and past life on your chronic pain.
For More Information
For more information on whole person pain care, read Dr. Wayne Jonas’ Guide to Optimizing Treatment through Integrative Health for People Living with Pain, available at drwaynejonas.com/painguide
CONCLUSION
Pain is the most common reason for doctor visits. And yet it is one of the most challenging medical conditions to treat, in part because it is so subjective and individualized. You and your friend might have the exact same diagnosis and yet feel the pain in completely different ways. That’s why it’s so important to remember that your pain is real and that you deserve the right treatment.
Finding the right combination of approaches to manage and reduce your pain can be a frustrating process. Thus, I urge you to be patient and to refuse to allow anyone to dismiss your pain. I also urge you to seek help from a variety of practitioners—both allopathic and complementary—in your search for pain relief and follow a holistic approach.
While they may not be able to completely cure your pain, the right mix of modalities, together with your commitment to doing your part, should definitely be able to reduce the frequency and severity and return you to the quality of life you deserve.
What You Can Do Now
- Focus on self-care—What works for you now?
- Find your meaning—What matters to you?
- Ask provider to do an Integrative Visit and HOPE Note—Explore how the areas of your life impact your health. (Learn more at drwaynejonas.com/hope)
- Develop your own health care team—Consider including traditional, complementary & alternative providers, and health coaches
REFERENCES
- Nahin RL. Estimates of pain prevalence and severity in adults: United States, 2012. J Pain. 2015;16(8):769-780.
- Institute of Medicine. Relieving Pain in America: A Blueprint for Transforming Prevention, Care, Education, and Research. 2011.
- Hurley RW, Adams MC. Sex, gender, and pain: an overview of a complex field. Anesth Analg. 2008;107(1):309-317.
- Aubrun F, Salvi N, Coriat P, Riou B. Sex- and age-related differences in morphine requirements for postoperative pain relief. Anesthesiology. 2005;103(1):156-160.
- Bijur PE, Esses D, Birnbaum A, Chang AK, Schechter C, Gallagher EJ. Response to morphine in male and female patients: analgesia and adverse events. Clin J Pain. 2008;24(3):192-198.
- Gear RW, Miaskowski C, Gordon NC, Paul SM, Heller PH, Levine JD. Kappa-opioids produce significantly
greater analgesia in women than in men. Nat Med. 1996;2(11):1248-1250. - Mogil JS, Bailey AL. Sex and gender differences in pain and analgesia. Prog Brain Res. 2010;186:141-157.
- Gijsbers K, Nicholson F. Experimental pain thresholds influenced by sex of experimenter. Percept Mot Skills.
2005;101(3):803-807. - Chou R, Ballantyne J, Fanciullo G, Fine P, Miaskowski C. Research gaps on use of opioids for chronic noncancer pain: findings from a review of the evidence for an American Pain Society and American Academy of Pain Medicine clinical practice guideline. J Pain. 2009;10(2):147-159.
- Vincent K, Tracey I. Hormones and their Interaction with the Pain Experience. Reviews in Pain. 2008;2(2):20-24.
- Amandusson A, Blomqvist A. Estrogenic influences in pain processing. Front Neuroendocrinol. 2013;34(4):329-349.
- Smith CA, Collins CT, Cyna AM, Crowther CA. Complementary and alternative therapies for pain management in labour. The Cochrane database of systematic reviews. 2006(4):Cd003521.
- Ivković N, Racic M, Lecic R, et al. Relationship Between Symptoms of Temporomandibular Disorders and Estrogen Levels in Women With Different Menstrual Status. J Oral Facial Pain Headache. 2018;Epub ahead of print.
- Craft RM, Mogil JS, Aloisi AM. Sex differences in pain and analgesia: the role of gonadal hormones. Eur J Pain. 2004;8(5):397-411.
- Nault T, Gupta P, Ehlert M, et al. Does a history of bullying and abuse predict lower urinary tract symptoms,
chronic pain, and sexual dysfunction? Int Urol Nephrol. 2016;48(11):1783-1788. - Jablonska B, Soares JJ, Sundin O. Pain among women: associations with socio-economic and work conditions. Eur J Pain. 2006;10(5):435-447.
- Centers for Disease and Control. Drug overdose deaths in the United States continue to increase in 2015. 2017;
https://www.cdc.gov/drugoverdose/epidemic/index.html. Accessed September 20, 2017. - Centers for Disease Control and Prevention. Prescription Painkiller Overdoses: A Growing Epidemic, Especially Among Women. 2013; http://www.cdc.gov/vitalsigns/prescriptionpainkilleroverdoses/index.html. Accessed March 20, 2018.
- Office on Women’s Health. Final Report: Opioid Use, Misuse, and Overdose in Women. July 2017 https://www.womenshealth.gov/files/documents/final-report-opioid-508.pdf. Accessed March 21, 2018.
- Quintiles IMS. An Analysis of the Impact of Opioid Overprescribing in America. Pacira Pharmaceuticals; September 2017 http://www.planagainstpain.com/wp-content/uploads/2017/09/PlanAgainstPain_USND.pdf. Accessed March 16, 2018.
- Gomez-Pomar E, Finnegan LP. The Epidemic of Neonatal Abstinence Syndrome, Historical References of Its’ Origins, Assessment, and Management. Frontiers in pediatrics. 2018;6:33.
- Sanlorenzo LA, Stark AR, Patrick SW. Neonatal abstinence syndrome: an update. Curr Opin Pediatr. 2018;30(2):182-186.
- Centers for Disease Control and Prevention. Guideline for Prescribing Opioids for Chronic Pain: Recommendations. 2017 https://www.cdc.gov/drugoverdose/prescribing/guideline.html.
- Hoffman DE, Tarzian A. The Girl Who Cried Pain: A Bias Against Women in the Treatment of Pain. J Law Med Ethics. 2001;29(1):13-27.
- Chen Esther H, Shofer Frances S, Dean Anthony J, et al. Gender Disparity in Analgesic Treatment of Emergency Department Patients with Acute Abdominal Pain. Acad Emerg Med. 2008;15(5):414-418.
- Huntington A, Gilmour JA. A life shaped by pain: women and endometriosis. J Clin Nurs. 2005;14(9):1124-1132.
- National Pain Report, For Grace. Women in Pain Survey. 2015; https://www.surveymonkey.com/results/SM-P5J5P29L/. Accessed March 26, 2018.
- Breuer B, Cruciani R, Portenoy RK. Pain management by primary care physicians, pain physicians, chiropractors, and acupuncturists: a national survey. South Med J. 2010;103(8):738-747.
- Martin BI, Gerkovich MM, Deyo RA, et al. The association of complementary and alternative medicine use and health care expenditures for back and neck problems. Med Care. 2012;50(12):1029-1036.
- Relief for your aching back: what worked for our readers. Consum Rep. March 17, 2017. http://www.consumerreports.org/cro/2013/01/relief-for-your-aching-back/index.htm. Accessed June 12, 2017.
- Vickers AJ, Cronin AM, Maschino AC, et al. Acupuncture for chronic pain: individual patient data meta-analysis. Arch Intern Med. 2012;172(19):1444-1453.
- American Massage Therapy Association. Consumer Views & Use of Massage Therapy. 2017; https://www.amtamassage.org/research/Consumer-Survey-Fact-Sheets.html. Accessed June 7, 2017.
- Morley S, Williams A, Hussain S. Estimating the clinical effectiveness of cognitive behavioural therapy in the
clinic: evaluation of a CBT informed pain management programme. Pain. 2008;137(3):670-680. - Fricton J, Gatchel RJ, Lawson KL, Whitebird R. Transformative Care for Chronic Pain and Addiction.
Practical Pain Management. October 2, 2017. https://www.practicalpainmanagement.com/treatments/psychological/transformative-care-chronic-pain-addiction. - Sharifzadeh Y, Kao MC, Sturgeon JA, Rico TJ, Mackey S, Darnall BD. Pain Catastrophizing Moderates Relationships between Pain Intensity and Opioid Prescription: Nonlinear Sex Differences Revealed Using a Learning Health System. Anesthesiology. 2017;127(1):136-146.
- Majeed MH, Sudak DM. Cognitive Behavioral Therapy for Chronic Pain-One Therapeutic Approach for the Opioid Epidemic. J Psychiatr Pract. 2017;23(6):409-414.
- Schutze R, Rees C, Smith A, Slater H, Campbell JM, O’Sullivan P. How Can We Best Reduce Pain Catastrophizing in Adults With Chronic Noncancer Pain? A Systematic Review and Meta-Analysis. J Pain. 2018;19(3):233-256.
- McDade TW, Hawkley LC, Cacioppo JT. Psychosocial and behavioral predictors of inflammation in middle-aged and older adults: the Chicago health, aging, and social relations study. Psychosom Med. 2006;68(3):376-381.
- Cacioppo JT, Hawkley LC. Social isolation and health, with an emphasis on underlying mechanisms. Perspect Biol Med. 2003;46(3 Suppl):S39-52.
- Pepe L, Milani R, Di Trani M, Di Folco G, Lanna V, Solano L. A more global approach to musculoskeletal pain: expressive writing as an effective adjunct to physiotherapy. Psychol Health Med. 2014;19(6):687-697.
- Trompetter HR, Bohlmeijer ET, Veehof MM, Schreurs KM. Internet-based guided self-help intervention for chronic pain based on Acceptance and Commitment Therapy: a randomized controlled trial. J Behav Med. 2015;38(1):66-80.
- Koopman C, Ismailji T, Holmes D, Classen CC, Palesh O, Wales T. The effects of expressive writing on pain,
depression and posttraumatic stress disorder symptoms in survivors of intimate partner violence. J Health Psychol. 2005;10(2):211-221. - Redwine LS, Henry BL, Pung MA, et al. Pilot Randomized Study of a Gratitude Journaling Intervention on Heart Rate Variability and Inflammatory Biomarkers in Patients With Stage B Heart Failure. Psychosom Med. 2016;78(6):667-676.
- Trivedi MH. The Link Between Depression and Physical Symptoms. Prim Care Companion J Clin Psychiatry. 2004;6(suppl 1):12-16.
- Smith CA, Levett KM, Collins CT, Crowther CA. Relaxation techniques for pain management in labour. The Cochrane database of systematic reviews. 2011(12):Cd009514.
- Bonapace J, Gagne GP, Chaillet N, Gagnon R, Hebert E, Buckley S. No. 355-Physiologic Basis of Pain in Labour and Delivery: An Evidence-Based Approach to its Management. J Obstet Gynaecol Can. 2018;40(2):227-245.
- Meriggiola MC, Nanni M, Bachiocco V, Vodo S, Aloisi AM. Menopause affects pain depending on pain type and characteristics. Menopause. 2012;19(5):517-523.
- Srikanth VK, Fryer JL, Zhai G, Winzenberg TM, Hosmer D, Jones G. A meta-analysis of sex differences prevalence, incidence and severity of osteoarthritis. Osteoarthritis Cartilage. 2005;13(9):769-781.
- Kozinoga M, Majchrzycki M, Piotrowska S. Low back pain in women before and after menopause. Przeglad menopauzalny = Menopause review. 2015;14(3):203-207.
- Martin VT, Pavlovic J, Fanning KM, Buse DC, Reed ML, Lipton RB. Perimenopause and Menopause Are Associated With High Frequency Headache in Women With Migraine: Results of the American Migraine Prevalence and Prevention Study. Headache. 2016;56(2):292-305.
- Monaco K. https://www.medpagetoday.com/meetingcoverage/nams/68527. Menopause May Be Risk Period for Chronic Pain, Opioid Use. October 13, 2017. https://www.medpagetoday.com/meetingcoverage/nams/68527. Accessed March 25, 2018.
CONTRIBUTORS
The following individuals provided guidance in the creation of this paper, but the product is the work of the author and is not necessarily a reflection of the contributors’, nor their organizations’ opinions.
Maggie Buckley, MBA
Board of Directors, The Pain Community (paincommunity.org)
Buckley has been a volunteer patient advocate for more than 20 years while living with the chronic pain condition Ehlers-Danlos Syndrome.
Cynthia Toussaint
Founder and Spokesperson, For Grace, (forgrace.org)
Toussaint has been a leading voice for women living with chronic pain since 2002. She has been living with Complex Regional Pain Syndrome and several other auto-immune conditions for 35 years.
Dr. James Fricton
Dr. Fricton had post-doctoral training in pain at UCLA and has devoted his career to patient care and research in temporomandibular and orofacial pain disorders. He also serves as a Professor in the Department of Diagnostic and Surgical Sciences at the School of Dentistry at the University of Minnesota. Dr. Fricton has published and lectured extensively and is the author of TMJ and Craniofacial Pain: Diagnosis and Management, Myofacial Pain and Fibromyalgia, and Advances in Orofacial Pain and TMJ Disorders. He currently sees patients at the Minnesota Head & Neck Pain Clinic, whose mission is to provide high-quality, effective patient care for head and neck disorders through a multispecialty, interdisciplinary approach designed to reduce pain and improve function.
ABOUT THE AUTHOR – DR. WAYNE JONAS
Dr. Jonas is a practicing family physician, an expert in integrative health and whole person care delivery, and a widely published scientific investigator. Dr. Jonas is the president of Healing Works Foundation. Additionally, Dr. Jonas is a retired lieutenant colonel in the Medical Corps of the United States Army.
Dr. Jonas was the director of the Office of Alternative Medicine at the National Institutes of Health (NIH) from 1995-1999, and prior to that served as the Director of the Medical Research Fellowship at the Walter Reed Army Institute of Research. He is a Fellow of the American Academy of Family Physicians. His research has appeared in peer-reviewed journals, such as the Journal of the American Medical Association, Nature Medicine, Journal of Family Practice, Annals of Internal Medicine, and The Lancet. Dr. Jonas received the 2015 Pioneer Award from the Integrative Healthcare Symposium, the 2007 America’s Top Family Doctors Award, the 2003 Pioneer Award from the American Holistic Medical Association, the 2002 Physician Recognition Award of the American Medical Association, and the 2002 Meritorious Activity Prize from the International Society of Life Information Science in Chiba, Japan.
Topics: Chronic Pain | Trauma | Women